




In utero, urine production is a critical factor in maintaining normal amniotic fluid levels. When amniotic fluid levels are very low, lung development may be impaired. This can result in serious breathing difficulties requiring ventilation upon birth. Sometimes, these breathing difficulties can cause death.
Children with ARPKD often produce a very large volume of urine and need to urinate much more frequently than children with typical kidneys. Urine production in ARPKD children doesn’t slow down at night or when liquid intake is limited.
High blood pressure is common in children with ARPKD. Current information indicates that untreated high blood pressure can lead to kidney failure more quickly than if the blood pressure is kept within the normal range with medications.
Children with ARPKD also have a liver abnormality, congenital hepatic fibrosis (CHF), that may lead to liver and spleen enlargement.
In the liver, CHF can impede the return of blood from the intestine to the liver. This condition, called portal hypertension, can lead to swelling and increased pressure in the veins around the esophagus, stomach, and intestine.
If pressure and distension increase, the organs can rupture, leading to possibly life-threatening gastrointestinal bleeding.
In addition, portal hypertension can cause spleen enlargement and hypersplenism, resulting in low red blood cell, white blood cell, and platelet counts.
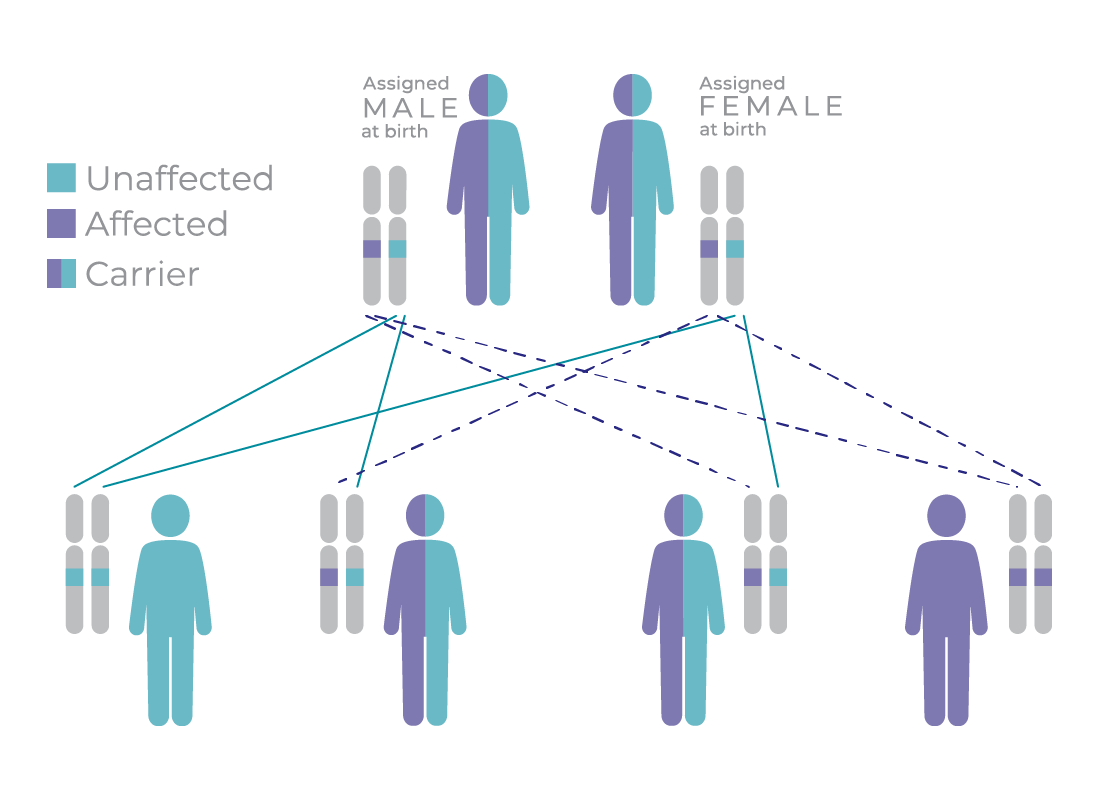
ARPKD genetic implications
This diagram demonstrates the rate at which ARPKD can be passed down from parents to children.
If two carrier parents have a child, there is a 25% chance their child will be completely unaffected, a 50% chance they will be a carrier of ARPKD, and a 25% chance they will be diagnosed with ARPKD.
FAQs
Find answers to the most commonly asked questions.
Where can I find more resources?

Search by keyword or select a topic to access reports, read articles, and watch webinars on ARPKD, ADPKD, and more.
Where can I find more information about the Centers of Excellence Program?
Discover more about PKD Foundation Centers of Excellence and download information you can share with your care team.
If your child has been diagnosed with ARPKD, learn more with our resources.
Get the latest information on treating PKD.
Sign up and get notified when there are clinical studies in your area.